

LEMBERT SUTURE
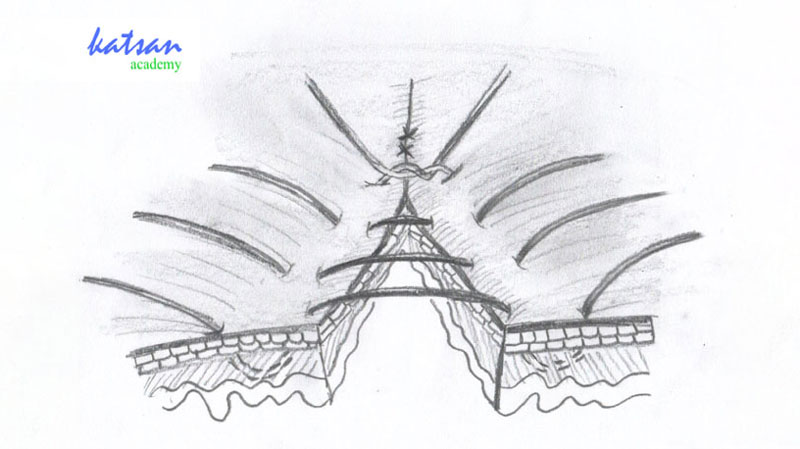 Figure 1 Interrupted Lembert Suture
Figure 1 Interrupted Lembert Suture Figure 2 Running Lembert Suture
Figure 2 Running Lembert Suture Figure 3 Czerny-Lembert Suture
Figure 3 Czerny-Lembert SutureLEMBERT SUTURE
Antoine Lembert, who carried out his operations in France in the early 1800s, starts a series of attempts to overcome some of the problems he faced during suturing the intestine. He stated that the quality of muco-mucosal sutures is low and sero-seroous sutures should be preferred over this type of suture
Later in 1826, he based his two-layered inversion suturing technique, which he developed for both anastomotic and intestine operations, on two principles:
1) The sutures should be placed in the submucosa due to its substantial strength.
2) The serous membrane should be accurately brought to the edge of the wound circumferentially.
The peculiarity of the Lembert suture is that by bending the serous surfaces, performing interrupted or running muscle-serous suturing with separate entrances and turning the edges of the wound into the intestinal lumen.
These principles, which were later slightly modified by Czerny and Connell, form the basis of modern principles, most of which are based on gastrointestinal anastomosis.
Figure 1 Interrupted Lembert Suture
Lembert suture is the simplest technique that can be used for the internal organs, performed relatively quickly. It inverts lips of the wound and never passes through the mucosa, so lowers the probability of the contamination. It consists of 7 basic steps:
- The needle is placed perpendicular to the epidermis at a distance of about 8 mm from the edge of the wound.
- With precise wrist movements, the needle is rotated under the surface of the dermis and the needle tip is removed 2 mm far from the wound edge on the ipsilateral side of the skin.
- The needle penetrates the skin perpendicular to the skin 2 mm far from the opposite side of the wound without touching the incision.
- The needle is turned under the dermis surface and leaves the skin 8 mm far from the incision. Thus, the reverse of the transaction on the other side has repeated.
- If the suture is to be made intermittently (Figure 1), it is gently knotted and cut. The process is repeated throughout the incision.
- If it is planned to be thrown continuously (Figure 2), the procedures are repeated until the end of the wound, starting with the first entry point, and the wound is closed by throwing the knot.
- Care is taken to minimize tension throughout the epidermis and prevent excessive narrowing of the wound edges during knotting.
Figure 2 Running Lembert Suture
This technique has been developed for intestinal suturing purposes from the outset where inversion is desired and really necessary. For this reason, it is not recommended to use in inversion undesired closure processes. It may cause stenosis in the intestine.
As with any transepidermal technique, this approach can cause post-operative scars; timely removal of sutures helps to reduce this risk, and using fast-absorbing sutures may also be a reasonable option.
No suture material traverses through the cut/wound, thereby reducing the risk of foreign body reaction, resulting in effective wound healing.
This technique does not contribute to the conjunction of the epidermal tip. Therefore, it is ideal to use after placing dermal sutures that effectively align the wound edges for more effective healing.
Many surgeons, who are aware of the shortcomings mentioned in the Lembert technique, have developed approaches to increase the safety of sutures and used this technique for different applications.
Czerny-Lembert Suture
Although he is known for his expertise in the field of oncology and gynecology, Vincenz Czerny, a versatile surgeon, has many contributions to the science of medicine and surgery. Important contributions to the surgical field of the German scientist include hernia operations, abdominal surgery, and vaginal hysterectomy. It is also considered the ancestor of cosmetic breast surgery. Most importantly, he acknowledged that surgery alone cannot control cancer and developed concepts for multimodality treatment.
A modification of the Lembert suture, which he developed as a result of his studies for intestinal and gastric anastomosis while he was working as a Professor at the Heidelberg Surgery Department in the early 1900s, was designed to overcome his predecessor’s lack of strength.
In the Czerny-Lembert intestinal suture, the needle first enters the serosa, passes through the submucosa or muscular, and then enters the submucosa or muscular of the opposite side and exits from the serosa. In this way, the first row of the suture is created and the Lembert suture is formed at the top of the incision and the wound is closed. This technique can be summarized briefly as a total of two rows of Lembert suture formed at the top and bottom of the incision (Figure 3).
Figure 3 Czerny-Lembert Suture
Mert Çeltikoğlu
Quality Assurance Chief



Frequently Asked Questions (FAQ) About PDO Barbed Sutures
As PDO barbed sutures become increasingly popular in aesthetic, dental, and surgical fields, healthc
Best Practices for Using PDO Barbed Sutures
PDO barbed sutures are transforming surgical routines across specialties thanks to their knotless cl
Absorption Timeline and Tissue Interaction of PDO Barbed Sutures
One of the key advantages of PDO (Polydioxanone) barbed sutures lies in their predictable absorption